Abscess in Stomach Internal Infection Emergency
- 1.
“Oi—Is That Just a Dodgy Burger… or Something Proper Wrong?” Recognising the First Whispers of an abscess in stomach
- 2.
From Grumble to Geyser: How an abscess in stomach Escalates When Left to Its Own Devices
- 3.
The Usual Suspects: Pinpointing the Main Cause of Abscess in the Abdomen
- 4.
“It Feels Like a Rugby Ball’s Lodged in Me Ribs”—What an abscess in stomach Actually *Feels* Like
- 5.
Imaging the Invisible: How Scans and Bloods Reveal the Hidden abscess in stomach
- 6.
Drain or Die? Navigating the Treatment Labyrinth for an abscess in stomach
- 7.
“But He’s Only Five!” — Tailoring Care for an abscess in stomach in Children
- 8.
Prevention Isn’t Paranoia: Simple Habits That Slash Your Risk of an abscess in stomach
- 9.
Myth vs. Muck: Busting Folk Beliefs About the abscess in stomach
- 10.
Living Beyond the Pus: Recovery, Relapse, and When to Ring the Alarm Again
Table of Contents
abscess in stomach
“Oi—Is That Just a Dodgy Burger… or Something Proper Wrong?” Recognising the First Whispers of an abscess in stomach
Ever woken up feelin’ like ye’ve wrestled a tumble dryer—and lost? Belly tight. Slightly warm to the touch. Maybe a low-grade fever that makes ye think, ‘Blimey, did I leave the oven on—or is me core just tryin’ to boil a kettle?’ That, dear reader, might not be indigestion. That could be the *very first murmur* of an abscess in stomach. Not the dramatic, Hollywood-style rupture (yet)—but the quiet, simmering sort that *really* doesn’t fancy being ignored. Early signs? Localised tenderness—press *just there*, near the upper-left or lower-right quadrant, and ye wince like ye’ve stubbed yer toe on a Lego brick at 3 a.m. Accompanied by nausea, bloating, and a vague sense ye’re carryin’ a rogue hot water bottle nobody asked for. And no—Gaviscon won’t cut it. Sorry, love.
From Grumble to Geyser: How an abscess in stomach Escalates When Left to Its Own Devices
Here’s the thing about an abscess in stomach: it’s not shy. Give it time, and it’ll throw a full-on rave—complete with flashing lights (fever spikes), bass-heavy thumps (palpitations from sepsis), and uninvited guests (bacteria on the loose). Untreated, that little pocket of pus can expand, press on the diaphragm (hello, hiccups that sound like a startled goose), or—*gulp*—rupture into the peritoneal cavity. That’s when ye go from “mild discomfort” to A&E in a heartbeat. Stats? Roughly 12–18% of intra-abdominal abscesses lead to septic shock if diagnosis is delayed beyond 72 hours. Not ideal when yer GP’s got a six-week waitlist and ye’re tryin’ to decide between paracetamol and a prayer.
The Usual Suspects: Pinpointing the Main Cause of Abscess in the Abdomen
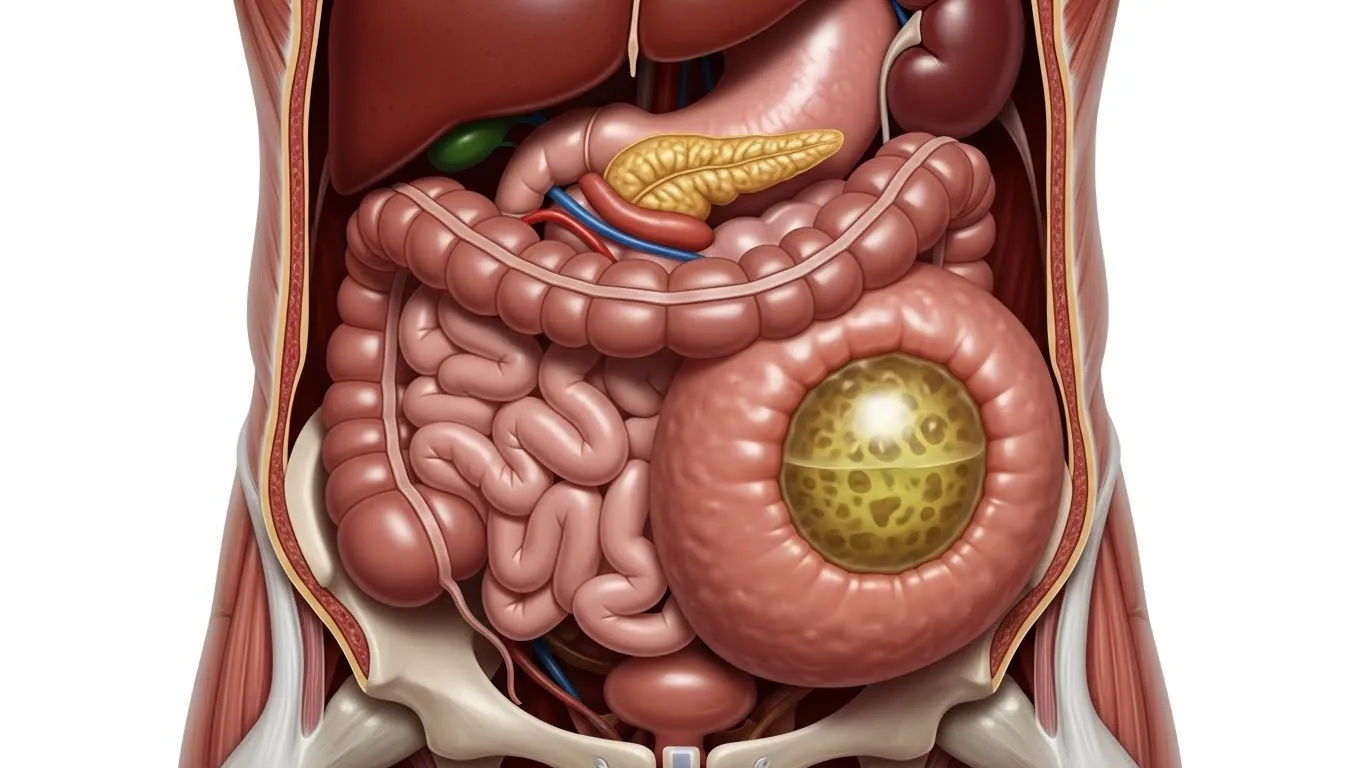
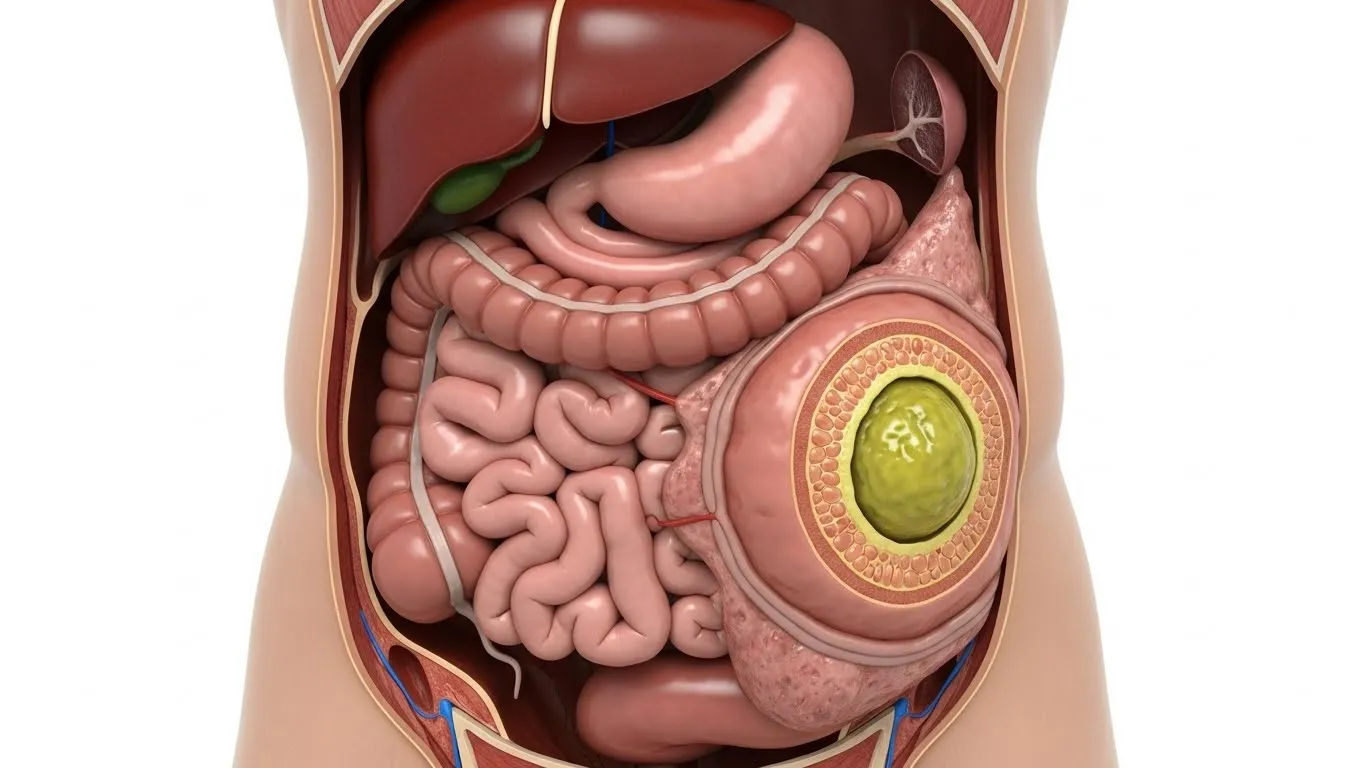
So—what *starts* an abscess in stomach? Spoiler: it’s rarely one villain. More like a gang of opportunists. Top of the list? Perforated appendicitis—the OG abscess starter pack. Then there’s diverticulitis (those pesky pouches in the colon get grumpy, inflamed, and *pop*), post-op complications (especially after bowel surgery), and—yes—penetrating trauma (think: bar brawl, rusty fence, or that time ye tried DIY plumbing *and* kebab consumption in the same hour). Oh, and don’t overlook *dental origins*: a tooth infection can seed bacteria into the bloodstream—travel south—and settle in quietly, like an uninvited houseguest who brings mould spores. The *main cause of abscess*? Honestly? A breach in the gut’s defences + delayed immune response. Nature’s version of “leave the back door open, and *of course* the raccoons’ll move in.”
“It Feels Like a Rugby Ball’s Lodged in Me Ribs”—What an abscess in stomach Actually *Feels* Like
Describing an abscess in stomach by sensation? Let’s get poetic. Imagine a hot pebble, wrapped in cling film, buried deep in yer abdomen—*throbbing* on a 90-second loop. It’s not sharp pain; it’s *dull, constant, insistent*—like a bassline ye can’t switch off. Cough? Feels like someone’s twistin’ a corkscrew near yer spleen. Lie flat? Pressure mounts. Sit up? Slight relief—but now yer back aches. Some report a “fullness” no amount of burping fixes. Others say it’s like carryin’ a water balloon filled with warm custard—*wobbly, heavy, and deeply suspicious*. And if it’s near the liver? Ye might feel referred pain in the right shoulder—because bodies love a bit of misdirection. “What does an abscess in stomach feel like?” In short: like yer insides are *holding a grudge*.
Imaging the Invisible: How Scans and Bloods Reveal the Hidden abscess in stomach
You can’t *see* an abscess in stomach—not without help. That’s where tech steps in, all calm and clever. Ultrasound? Quick, cheap, great for superficial pockets—but limited by gas and body habitus (sorry, blokes with a proper “Dad bod”). CT scan? The gold standard. Shows size, location, even if it’s walled off (like a tiny, angry fortress). And bloods? Oh, they *talk*. Elevated CRP? Sky-high white count? Ferritin creeping up like a nosy neighbour? All red flags. Here’s a snapshot of typical markers in confirmed cases:
| Marker | Normal Range | Average in abscess in stomach |
|---|---|---|
| WBC (x10⁹/L) | 4.0–11.0 | 14.5–22.0 |
| CRP (mg/L) | <5 | 85–210 |
| Temperature (°C) | 36.1–37.2 | 38.3–39.6 |
Drain or Die? Navigating the Treatment Labyrinth for an abscess in stomach
Right—ye’ve got the diagnosis. Now what? Contrary to TikTok “detox tea” trends, an abscess in stomach won’t vanish with lemon water and affirmations. Nope. Rule one: *don’t* squeeze. Rule two: *do* get imaging-guided drainage—either percutaneously (needle through the skin, ultrasound in hand) or laparoscopically (tiny keyhole incisions, camera in). Antibiotics? Essential—but *never* enough alone. Pus needs exit. Studies show success rates jump from ~55% (antibiotics only) to >92% when drainage’s added. And ye’ll likely be on IV abx for 7–14 days *after*—£800–£1,200 on the NHS tab if outpatient, more if admitted. Not fun. But far cheaper than sepsis.
“But He’s Only Five!” — Tailoring Care for an abscess in stomach in Children
Kids don’t do subtlety. An abscess in stomach in a toddler might show as *refusal to walk* (pain worsens with movement), high-pitched crying, or that eerie “quiet lethargy” that makes yer blood run cold. Common culprits? Appendicitis (peak age 10–12), perforated Meckel’s diverticulum, or—heartbreakingly—complications from untreated dental infections. How to treat abscess in kids? Same principles: drainage + antibiotics—but with *extra* gentleness. Paediatric interventional radiologists use smaller catheters (2–5 Fr, not 8–10), and abx dosing’s weight-based (amoxicillin-clavulanate remains first-line, unless MRSA suspected). Recovery? Kids bounce back *fast*—if caught early. Delay? Risk of growth plate involvement, malnutrition, even fistulae. So if yer nipper’s doubled over, pale, and won’t touch their favourite crisps? *Don’t wait.* Trust yer gut—often sharper than any scan.
Prevention Isn’t Paranoia: Simple Habits That Slash Your Risk of an abscess in stomach
Look—we can’t promise immunity. But we *can* stack the odds. First: treat dental infections promptly. A £50 filling beats a £5,000 hospital stay. Second: *don’t ignore abdominal pain that lingers*. “Wait-and-see” works for hangnails—not gut perforations. Third: post-op, *follow discharge advice like yer life depends on it* (because sometimes, it does). Hydration? Non-negotiable. Fibre? Your colon’s best mate. And *please*—if ye’ve got Crohn’s or diverticular disease, stick to the med plan. Skipping mesalazine to “save a fiver” isn’t thrifty—it’s Russian roulette with yer insides. Prevention isn’t perfect. But it’s *far* cheaper—and kinder—than cure.
Myth vs. Muck: Busting Folk Beliefs About the abscess in stomach
Let’s clear the air, shall we? ❌ *“Abscesses need to ‘ripen’ before draining.”* → Nope. Delay = bigger abscess = higher rupture risk. ❌ *“Warm compresses will draw it out.”* → Works for skin boils. For deep abscess in stomach? Might as well whistle at a storm. ❌ *“Antibiotics alone will dissolve it.”* → They’ll calm the riot—but the *building* (pus cavity) stays. Needs evacuation. ❌ *“Only dirty people get them.”* → Rubbish. Elite athletes, surgeons, toddlers—*anyone* with a breached barrier’s at risk. As one old GP in Newcastle told us: *“An abscess isn’t a moral failing—it’s a plumbing failure.”* And even the best pipes leak sometimes.
Living Beyond the Pus: Recovery, Relapse, and When to Ring the Alarm Again
Drainage done. Antibiotics ticking along. Ye’re home, wrapped in a blanket, sippin’ tea like ye’ve just survived a heist. Good. But recovery’s a *marathon*, not a sprint. Expect fatigue for 2–4 weeks. Gentle walks—not gym seshes. Diet? Start bland (rice, toast, stewed apples), then ease back in. Watch for red flags: *returning fever*, new rigidity, vomiting bile. That’s not “just a bug”—that’s possible recurrence or secondary infection. And if ye’ve had one abscess in stomach, yer risk of another rises ~15–20% in 12 months—especially with underlying GI conditions. So stay sharp. Keep notes. And when in doubt? Call yer GP *before* ye Google. For more practical wisdom, swing by Riding London, explore our Learn hub, or check out our guide on face swelling from tooth infection dental abscess—because infections love to travel, and knowledge’s the best passport.
Frequently Asked Questions
How serious is a stomach abscess?
An abscess in stomach is a medical emergency. Left untreated, it can lead to sepsis, multi-organ failure, or rupture—carrying a mortality rate of up to 10–15% in delayed cases. Early intervention (drainage + antibiotics) reduces risk drastically, but time is critical.
What does an abscess feel like in your stomach?
An abscess in stomach typically presents as deep, constant, dull pain—often localised but worsening with movement, coughing, or lying flat. Accompanying symptoms include fever, nausea, bloating, and sometimes referred pain to the shoulder or back. It feels less like cramp, more like a hot, heavy pressure that *won’t shift*.
What is the main cause of abscess?
The main cause of abscess is bacterial invasion following a breach in mucosal or skin barriers. In the abdomen, common triggers include perforated appendicitis, diverticulitis, post-surgical leaks, or haematogenous spread (e.g., from dental infections). Polymicrobial flora—often *E. coli*, *Bacteroides*, and *Enterococcus*—dominate.
How to treat abscess in kids?
To treat an abscess in stomach in children, image-guided drainage (ultrasound/CT) is preferred, paired with IV antibiotics tailored to weight and likely pathogens. Oral step-down follows once afebrile and improving. Close monitoring for complications—like growth disturbance or fistula formation—is essential. Never delay: kids decompensate faster than adults.
References
- https://www.ncbi.nlm.nih.gov/books/NBK537062/
- https://www.sciencedirect.com/science/article/pii/S0002961020302456
- https://www.bmj.com/content/368/bmj.m152
- https://www.rch.org.au/clinicalguide/guideline_index/Intra_abdominal_abscess/